The equine breeding season is now in full swing which means that our vets have been busy scanning mares as well attending mares and foals for routine post-partum checks as well as unfortunately, in some cases, illness.
Many of you may wonder, if the birthing process proceeds uneventfully, why the need to check mare and foal postpartum. For the remainder of this piece we will explain why this is so important in a little more detail.
Following birth, the one, two, three ‘rule’ is important to remember-
- One: the foal should stand within one hour of birth
- Two: the foal should show ability to nurse within two hours of birth (most mares should have expelled their placenta within this timeframe also)
- Three: the foal should be actively nursing and consuming colostrum within three hours of birth.
If the above three timepoints are not achieved then a veterinary examination is warranted sooner rather than later. Otherwise if mare and foal are doing well, the above timepoints have been met and the mare has passed her placenta then a postpartum check should be performed within the first 24-36 hours following parturition (birthing). It is important to remove the placenta from the mare’s bed as soon as possible following expulsion and retain it for veterinary examination.
At the post-partum check, the attending vet will generally ask questions about the mare’s pregnancy and the birthing process. A full physical examination is subsequently performed on the foal whereby the attending vet will examine the foal’s heart, chest, joints, umbilicus and check for evidence of hernias. They will also check the foal’s mouth for cleft palate and ascertain it’s jaw alignment- has it an overshot/undershot jaw. Occasionally foals have turned in eyelids which results in their eyelashes rubbing the cornea (entropion) so it is also really important to check there is no evidence of this. We will generally check the foal’s nursing also.
It is highly recommended that a blood sample is taken to ascertain the foal’s IgG status. But what is this and why is it so important?
Foals are born immuno-naive which means that they are incredibly susceptible to infection should they consume inadequate quantities of colostrum (the mare’s first milk) or the mare’s colostrum is of insufficient quality. This ‘failure’ is known as ‘failure of passive transfer.’ If the mare has run milk for days on the lead up to birth, there is a distinct possibility that she will have lost the protective antibodies that would normally be concentrated in the colostrum. On the other hand, if the mare’s colostrum is of sufficient quality but the foal fails to consume sufficient quantities within the first 12 hours of life or so then the foal will consume and absorb insufficient amounts of antibodies. Both scenarios lead to failure of passive transfer. The foal’s gastrointestinal tract is capable of absorbing these antibodies most effectively during the first 12 hours of life but some absorption continues, albeit at a reduced amount, up until approximately 24 hours of age. The IgG blood test determines the foal’s antibody level. This simple blood test is performed on yard with results within a few hours at the latest. The best-case scenario is that results return indicating successful passive transfer but if test results indicate failure then the time postpartum determines the action required. If heading towards 24hrs plus postpartum, then a plasma transfusion is indicated. Your vet will discuss the most appropriate course of action with you.
It is equally as important to check the mare and her placenta as well as the foal. A full physical examination should be performed and the placenta checked. The mare’s perineal area should also be examined for birthing trauma. Finally, the mare’s bag (udder) should be checked and should be soft and well nursed. A hard, engorged bag is not normal and is often the first tell-tale sign that a foal is poorly and nursing insufficiently.
 A nerve block is the deposition of local anaesthetic into the area immediately surrounding a nerve body or ending. This stops the nerve from transmitting signals relating to pain back to the brain, hence pain is prevented or “blocked”. Practically, the term nerve blocking is often used to describe the placement of nerve blocks in the truest sense, and also the deposition of local anaesthetic into joints and into the tissue surrounding the spinal cord (an epidural), rather than around nerves.
A nerve block is the deposition of local anaesthetic into the area immediately surrounding a nerve body or ending. This stops the nerve from transmitting signals relating to pain back to the brain, hence pain is prevented or “blocked”. Practically, the term nerve blocking is often used to describe the placement of nerve blocks in the truest sense, and also the deposition of local anaesthetic into joints and into the tissue surrounding the spinal cord (an epidural), rather than around nerves.  The procedure involves observing the horse moving in a straight line, on circles on both reins and on firm and soft surfaces. This allows grading and characterisation of the lameness. A nerve block is then placed, stopping the sensation of pain in a specific area. Once this has had chance to take effect, the horse is once again observed moving as previously. Any substantial reduction of lameness can therefore be attributed to pain coming from within the area that has been desensitised by the nerve block. If the lameness is unchanged, it can be deduced that the source of pain is not within the blocked area of the limb, and further nerve blocks can be performed to desensitise other area of the limb until the source of lameness is known.
The procedure involves observing the horse moving in a straight line, on circles on both reins and on firm and soft surfaces. This allows grading and characterisation of the lameness. A nerve block is then placed, stopping the sensation of pain in a specific area. Once this has had chance to take effect, the horse is once again observed moving as previously. Any substantial reduction of lameness can therefore be attributed to pain coming from within the area that has been desensitised by the nerve block. If the lameness is unchanged, it can be deduced that the source of pain is not within the blocked area of the limb, and further nerve blocks can be performed to desensitise other area of the limb until the source of lameness is known.  Positioning
Positioning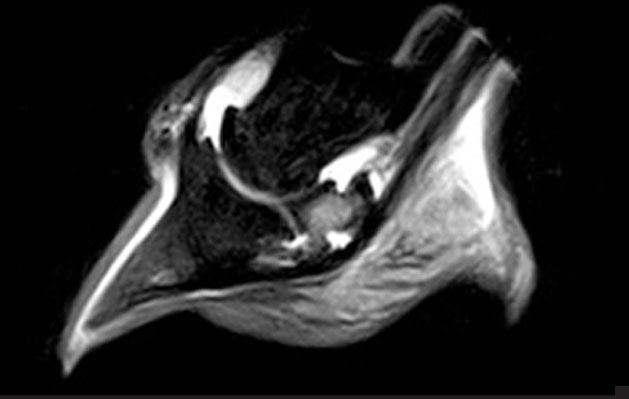 The scan takes around 2 – 4 hours, producing around 300-500 images at multiple angles of the limb or hoof, highlighting different types of tissue and pathology.
The scan takes around 2 – 4 hours, producing around 300-500 images at multiple angles of the limb or hoof, highlighting different types of tissue and pathology.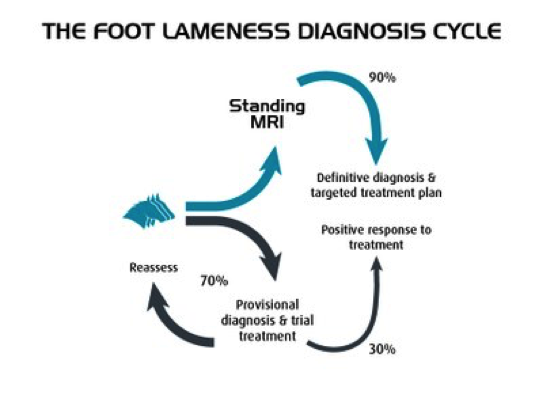
 Is it the same as a human MRI scanner?
Is it the same as a human MRI scanner?